Who uses sensed PACs to help diagnose the mechanism of tachycardia?
When used correctly, sensed PACs can be an extremely powerful diagnostic tool. Interpreting the response, however, can be challenging, particularly in a 1:1 short RP tachycardia, like the example shown above.
One key advantage of sensed PACs is their ability to differentiate typical AVNRT from junctional tachycardia. This distinction is especially important during the testing phase after slow pathway ablation. At this stage, isoprenaline is commonly administered, and junctional tachycardia may emerge and closely mimic typical AVNRT. Correctly identifying the mechanism here is critical, as it may determine whether additional ablation is required, and unnecessary ablation increases the risk of complications.
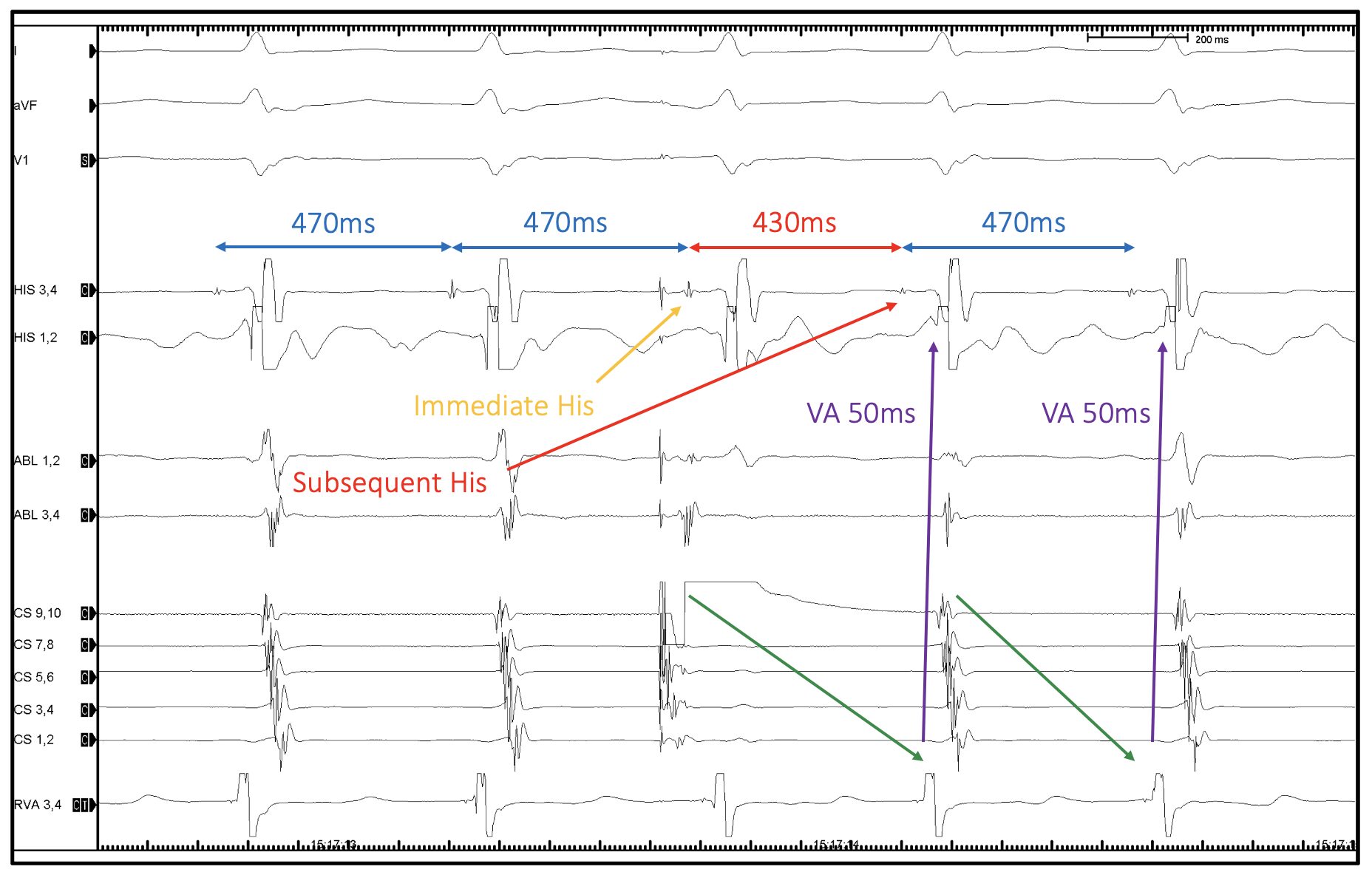
When performing this manoeuvre, the first step is to identify the immediate His and the subsequent His.
· The immediate His is the His signal directly following the pacing stimulus (orange arrow).
· The subsequent His is the next His signal (red arrow).
In typical AVNRT, the immediate His and the preceding H–H interval is unaffected, as ventricular depolarisation has already occurred via the antegrade slow pathway (blue calliper: 470ms).
So, what effect does a sensed PAC have on the AVNRT circuit?
First, the antegrade wavefront of the PAC collides with the retrograde fast pathway wavefront, terminating the re-entrant circuit. Second, the PAC engages the antegrade slow pathway earlier than expected due to its prematurity. This results in earlier ventricular depolarisation, effectively resetting the circuit. In this example, the subsequent H–H interval shortens to 430ms (red calliper), meaning the His has been advanced by 40ms. This response is diagnostic of re-entry and consistent with typical AVNRT.
Of note, the return VA interval is identical that of the SVT, further supporting AVNRT and excluding a focal atrial tachycardia with a long PR mechanism.
In some cases, an earlier PAC may also advance the immediate His. If this occurs and the tachycardia terminates, this is again diagnostic of re-entry and most consistent with AVNRT. In this scenario, the PAC wavefront again collides with the retrograde fast pathway but encounters refractory tissue in the slow pathway, preventing conduction. The tachycardia therefore terminates rather than resets.
If you want to develop a deeper understanding of sensed PACs, pacing manoeuvres, and the nuanced responses seen across different SVTs, CEPIA’s Graduate Diploma in Cardiac Electrophysiology explores these concepts in depth.
Using real EP tracings with practical interpretation we will help you master the quest for SVT diagnosis.