The use of sensed PACs during SVT is a valuable tool. However, you must be aware of when the results can give you conflicting results.
In this example, a sensed PAC is delivered during a long RP tachycardia with inverted P waves in lead II suggesting a low to high atrial activation. The atrial activation shows CS 7-8 earliest followed by CS 9-10 then His A.
Based on this, the differential includes:
- Atypical AVNRT
- Focal atrial tachycardia from a low atrial focus
- Orthodromic AVRT
It’s important to point out that unlike last week, we’re not using sensed PACs to differentiate typical AVNRT from junctional tachycardia, those mechanisms are already unlikely based on the tachycardia appearance and intervals. This time, the goal is to differentiate an AT from AVNRT & AVRT. The following steps outline how to do this.
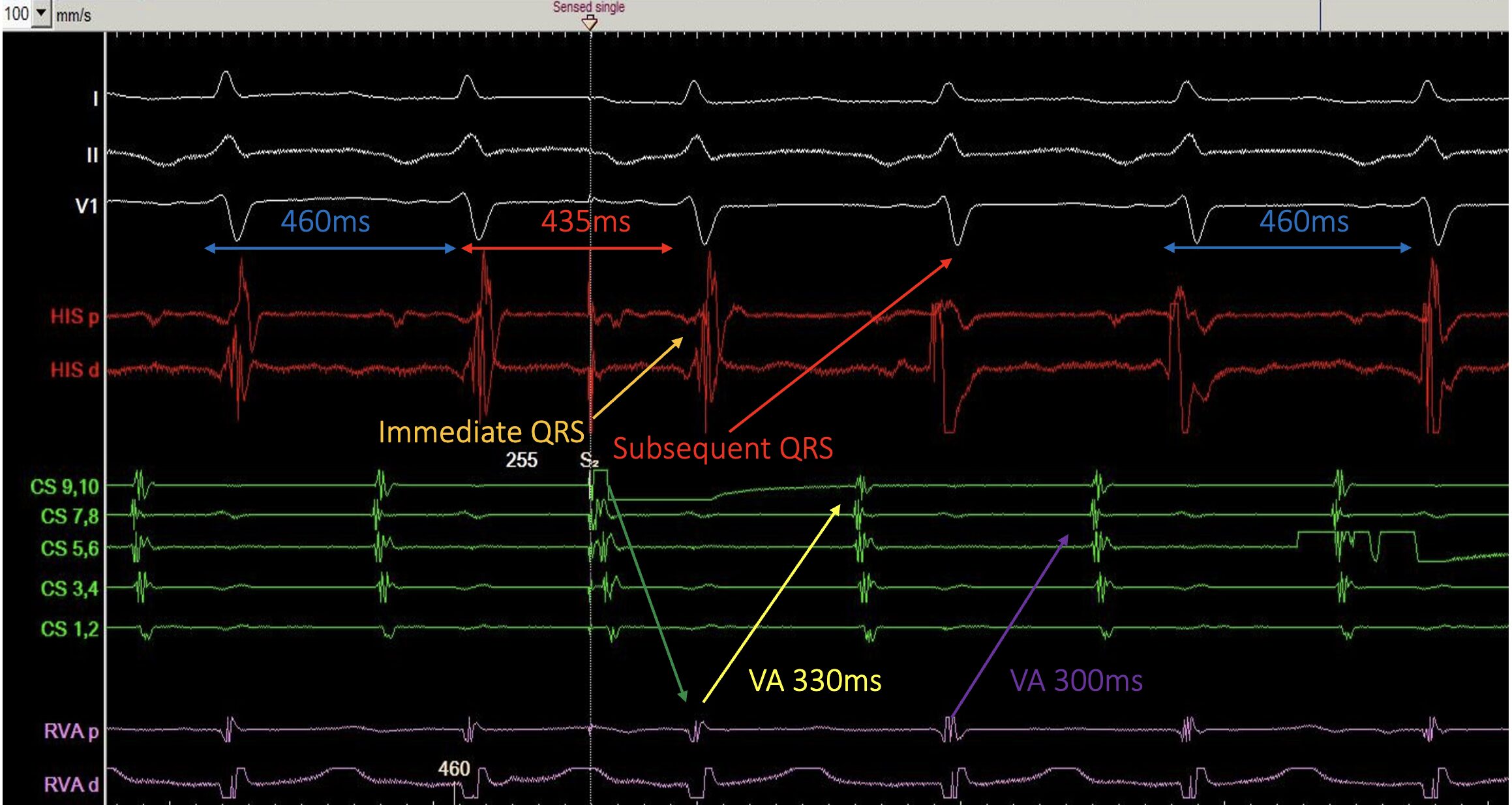
Step 1: Did the PAC advance the immediate His/QRS?
The PAC advances the immediate QRS from 460ms to 435ms (we’re using QRS as a surrogate because the His isn’t clearly seen). Advancing of the immediate His/QRS can occur in atypical AVNRT, AVRT, and focal AT so the advancement itself isn’t the discriminator. It simply means the response diagnostic.
Step 2: Is the return VA “hooked”?
Next, assess the return VA interval.
In a re-entrant mechanism, the retrograde wavefront returns to the atria via the same pathway, whether it’s during SVT or following the paced beat. So, the return VA should match the VA during SVT (i.e., it’s “hooked”).
In focal AT, the paced beat transiently suppresses the focus, and then the tachycardia resumes at its own intrinsic rate which often produces a different return VA (i.e., “not hooked”).
Here:
- Return VA post-PAC = 330ms (yellow arrow)
- VA during SVT = 300ms (purple arrow)
The VA is Not hooked.
Most of the time, this response points toward focal atrial tachycardia.
However, in around 5–6% of cases, you can see a “not hooked” VA response in atypical AVNRT as well and in this tracing, the P-wave morphology and activation pattern still fit with atypical AVNRT.
Why might atypical AVNRT look “not hooked”?
AVNRT circuits can be more complex than the classic teaching model. One plausible explanation here is that a PAC delivered from the CS ostium may partially conceal into the retrograde slow pathway, leaving the tissue incompletely recovered. This can slow the retrograde conduction during SVT, prolonging the return VA compared with the tachycardia VA. This creates a “not hooked” appearance despite re-entry.
Take-home message
Sensed PACs during long RP tachycardia are very helpful — but a “not hooked” VA does not automatically equal focal AT.
If you see this response, don’t stop at the PAC manoeuvre. Follow it with VOPD (and the rest of your pacing toolkit) to confirm the mechanism. In this case, the diagnosis was atypical AVNRT which was confirmed using VODP with a VAV response seen.
If you want to develop a deeper understanding of sensed PACs, pacing manoeuvres, and the nuanced responses seen across different SVTs, CEPIA’s Graduate Diploma in Cardiac Electrophysiology explores these concepts in depth.
We focus on real EP tracings, practical interpretation, and the clinical decision-making that matters in the lab.