Ventricular Overdrive Pacing: The King of Diagnostic Manoeuvres
When performing pacing manoeuvres during an SVT study, it is difficult to go past ventricular overdrive pacing (VODP). With this single intervention, multiple diagnostic elements can be assessed, often allowing the mechanism to be diagnosed immediately.
VODP provides insight into:
- Retrograde atrial activation:If ventricular pacing reproduces the same retrograde atrial activation seen during SVT, atrial tachycardia (AT) becomes unlikely. This is particularly useful in a four-catheter study with a catheter positioned in the high right atrium. This is less helpful if the AT focus is arising from near the atrial septum in which antegrade atrial activation looks similar to concentric retrograde atrial activation.
- Number of beats to entrainment:
Atrial entrainment must occur first and foremost, however, tachycardia does not need to persist post pacing to assess this response. The number of beats required to entrain can help differentiate AVNRT from AVRT. - Return sequence:Is the return sequence an ‘AV’ or ‘AAV’ response. This can help exclude an AT, however, this does not distinguish AVNRT from AVRT.
- Atrial involvement during pacing and termination:If tachycardia continues without the atria being depolarised by the pacing wavefront (i.e., VA dissociation) then AVRT can be excluded. If termination occurs without perturbing the atrial cycle length this can further clarify the mechanism.
- Post-pacing interval (PPI):
When pacing from the RV apex, a longer PPI–TCL suggests AVNRT, whereas a shorter interval suggests AVRT. This specific response is not used to differentiate an AT.
A strong grasp of VODP interpretation is fundamental to accurate SVT diagnosis.
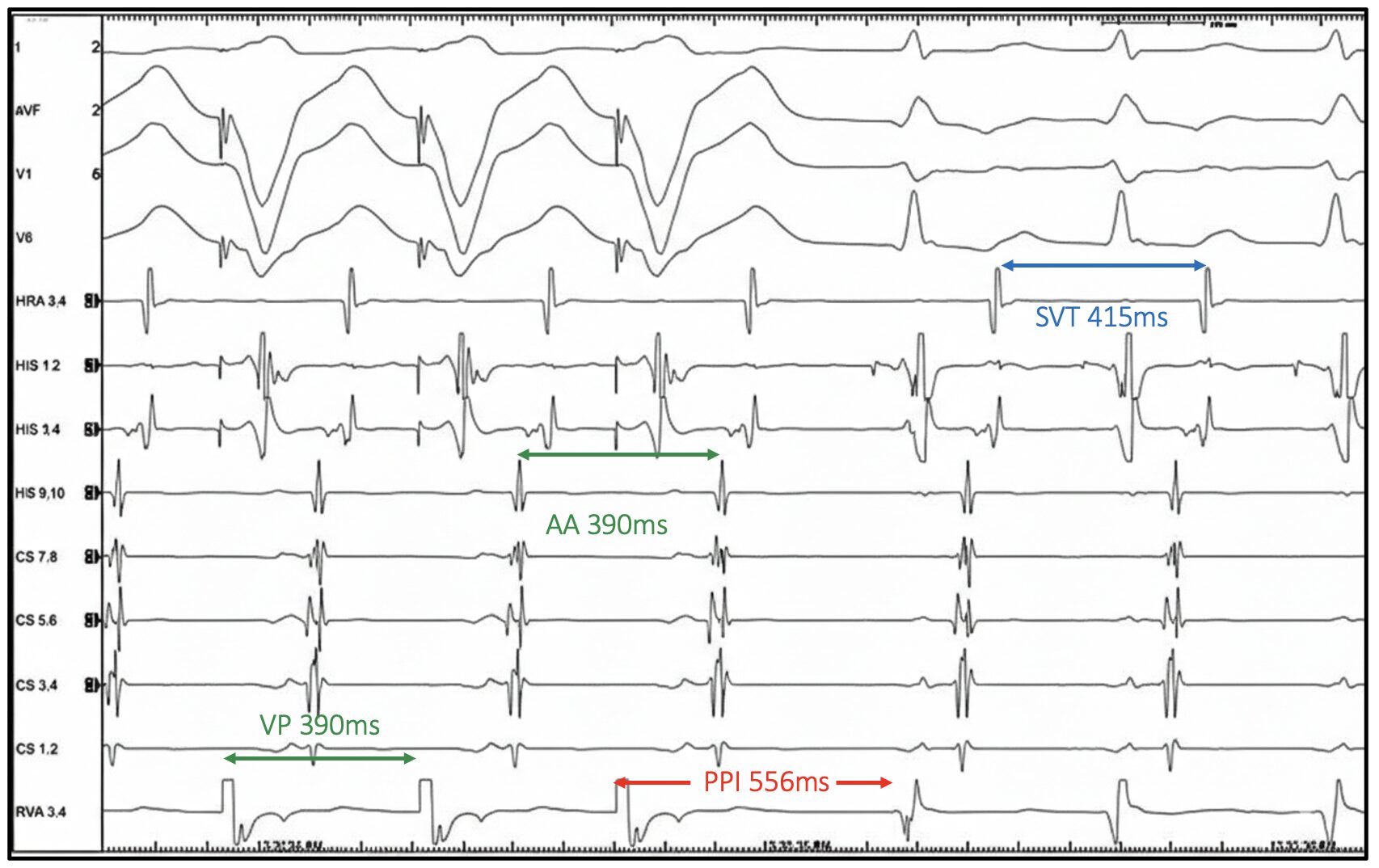
Let us examine the EGM above
The intrinsic tachycardia demonstrates:
- Narrow QRS
- 1:1 AV relationship
- A His preceding each QRS
Antidromic AVRT and VT can therefore be excluded. The atrial activation pattern will be revisited shortly.
VODP is delivered at 390ms, approximately 25ms faster than the tachycardia cycle length (TCL 415ms).
Was entrainment achieved?
Yes. The atria have been accelerated to the pacing cycle length and tachycardia persists following pacing.
Lets run through a few items that we can from the above checklist in no particular order:
Retrograde Atrial Activation
Retrograde atrial activation during VODP matches that seen during SVT. This supports a re-entrant mechanism and makes atrial tachycardia unlikely.
The activation pattern is eccentric, the order of atrial activation is as follows:
- Distal-to-proximal CS
- His A
- HRA
This pattern strongly suggests conduction over a left free wall accessory pathway.
However, rare mimics must be considered, including:
- Atypical AVNRT using an inferolateral left atrial (IL-LA) atrio-nodal pathway
- Left atrial focal tachycardia with a bystander accessory pathway.
As you can see, the activation pattern alone is not diagnostic.
Return Sequence
The return sequence demonstrates an AV response. An AV response excludes an atrial tachycardia.
The differential now narrows to either :
- Atypical AVNRT or
- Orthodromic AVRT
Initial PPI–TCL Assessment
PPI = 556ms, TCL = 415ms
PPI–TCL = 141ms
Traditional cut-offs using RVA pacing are as follows:
- >115ms = AVNRT
- <115ms = AVRT
A PPI – TCL of 141ms would suggest AVNRT in this case. But interpretation should not stop here. See the EGM below with additional callipers.

The Critical Step: Correcting for AH Prolongation
The return AH & AH during SVT have been measured and are as follows:
- Return AH = 245ms
- SVT AH = 190ms
There is a difference of 55ms. During faster RV pacing, there is concealed retrograde conduction into the AV node, therefore the AV node may exhibit decremental prolongation of AH afterwards i.e., its more fatigued post pacing. This artificially lengthens the measured PPI and may falsely suggest AVNRT as a result.
Therefore, the PPI must be corrected.
cPPI = PPI – TCL – (Return AH – SVT AH)
cPPI = 141ms – 55ms
cPPI = 86ms
A value of 86ms is now highly suggestive of AVRT and excludes AVNRT.
The corrected PPI – TCL cut-offs are below:
- >110ms = AVNRT
- <110ms = AVRT
Take home message:
- Always confirm atrial entrainment.
- An AV response excludes atrial tachycardia but does not distinguish AVNRT from AVRT.
- Atrial activation pattern alone is insufficient for diagnosis.
- Always assess the return AH and correct the PPI when necessary.
- An uncorrected PPI may lead to misdiagnosis.
Ventricular overdrive pacing remains the most powerful diagnostic manoeuvre in SVT but only when interpreted correctly.
If you want to develop a deeper understanding of the pacing manoeuvres, and the nuanced responses seen across different SVTs, CEPIA’s Graduate Diploma in Cardiac Electrophysiology explores these concepts in depth.
We focus on real EP tracings, practical interpretation, and the clinical decision-making that matters in the lab.
📚 100% online
🌍 Study anywhere, anytime
Visit CEPIA today and start your EP journey.